Get expert insights into cough science, monitoring and research

A decentralized feasibility study that delivered rich, real-world cough data without the scale, cost, or complexity of a trial or a market-research program.
About 50% of patients with refractory chronic cough go into full remission; they don’t have a chronic cough anymore. Over 80% experience a significant reduction in their symptoms.
4 March 2026
By Laurie Slovarp, PhD, CCC-SLP
Most of the patients I see in the clinic have been coughing for a very long time. They’ve seen multiple physicians, had lots of tests and treatments, and we are often at the end of that road. By the time they reach me, they’ve frequently been told there’s nothing else to try.
That’s almost never true.
There is a treatment for refractory chronic cough that works. Three randomized controlled trials support it; over 10 published studies confirm its effects; and a meta-analysis of the data all lead to the same conclusion: this therapy is more effective than anything else available for this condition. It’s safe. It’s inexpensive. And when patients access it early, within the first year of symptoms, it’s not unusual for their cough to be completely gone in a week. I’ve had patients whose seemingly ruinous cough resolved in a couple of days.
The treatment is called Behavioral Cough Suppression Therapy, or BCST. The name does not imply that their cough is behavioral in nature, as if it were a habit, but that the treatment is behavioral, requiring no medication. Despite BCST’s proven track record, most chronic cough patients have never heard of it.
Watch the full conversation between Dr. Laurie Slovarp and Hyfe CPO Reid Moorsmith on the science behind BCST and the future of chronic cough treatment.
Chronic cough has many causes. But in a large subset of patients, the cough is driven by a neurological condition called cough hypersensitivity. In these patients, the nervous system – primarily the brain– has become overprotective, interpreting things that are not a threat, such as a change in temperature, vibration in the throat from talking, or certain odor, as a threat to the lungs, and triggering a cough response. Over and over again. The cough reflex has essentially been reset to a very low threshold.
This is actually good news, because our brains are modifiable. BCST teaches patients to identify the urge to cough, resist it using specific breathing and swallowing techniques, and practice consistently. Over time, this retrains the nervous system to stop being overprotective, and the hypersensitivity can resolve.
About 50% of patients with refractory chronic cough go into full remission; they don’t have a chronic cough anymore. Over 80% experience a significant reduction in their symptoms. Unlike medications for cough, which essentially cover up the hypersensitivity, often come with side effects, and must be taken indefinitely, BCST directly targets the root cause.
This is the question I get asked most often, and the answer is frustratingly straightforward: awareness and access.
Cough hypersensitivity isn’t typically taught in medical school. Most general practitioners aren’t aware of it as a distinct condition, so they don’t even know to look for a treatment for it. The medical model has historically treated cough as a symptom of some other illness: find the illness, treat the illness. That’s still appropriate in many cases; but once a patient has developed cough hypersensitivity, treating whatever originally triggered it won’t usually resolve the cough. The hypersensitivity itself needs to be addressed.
Then there’s the specialist bottleneck. BCST is typically delivered by speech-language pathologists who specialize in voice and upper airway conditions, and we make up only about 3% of all SLPs. In the United States, there are probably no more than 200-300 speech pathologists who treat this condition. The estimates suggest 7 to 10 million Americans have refractory chronic cough, and up to 100 million people worldwide. Even if every physician knew to refer, there simply aren’t enough of us to treat all the people who would benefit from BCST.
My hope is that within the next five years, cough hypersensitivity is broadly recognized as a distinct disease, not just a symptom of something else, but a condition that needs its own treatment pathway. Physicians need to know it exists. While the American, European, British, and Australian clinical guidelines all suggest trying behavioral therapy to treat cough hypersensitivity, there is a lack of consensus across the recommendations about who should be referred for BCST and when that referral should be made. Additionally, the stated strength of evidence in support of BCST varies across the guidelines, with some guidelines suggesting it as a consideration after pharmaceutical interventions have failed, and others strongly recommending it as the first treatment after a diagnosis of RCC is made. Across the board, national guidelines should reflect the current state of the evidence, which at this point clearly shows that BCST is the most effective treatment for RCC. We also need to solve the access problem. That means training more clinicians, but it also means thinking creatively about how to deliver this therapy to people who don’t live near a specialist. Digital health tools are beginning to open that door, making it possible to extend BCST principles to patients who would otherwise have no one to turn to. That won’t replace the value of working with a skilled therapist, but for the millions of people who currently have no options, it could change everything.
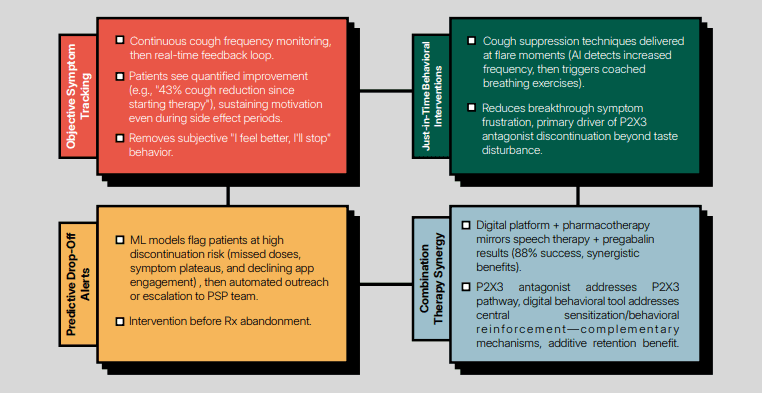
And we need better measurement. One of the historic challenges in cough treatment has been the inability to objectively track what’s happening between clinic visits. Research has shown time again that simply asking patients if they are better is not an accurate gauge. Tools for continuous, real-world cough monitoring are changing that, giving clinicians and researchers the data to measure outcomes, personalize treatment, and build the evidence base further.
What we observe in clinic is that when patients reach BCST early, outcomes are fastest. A long course of treatment is four to six weeks. Many patients improve significantly in two to three. In contrast, acid reflux is probably the most common suspected illness to be the cause for a chronic cough. The recommended treatment approach for acid reflux is a 2-3 month trial of anti-reflux medication. Yet, several studies have shown that, while anti-reflux medication typically resolves acid reflux symptoms like heartburn, it rarely corrects the cough. This begs the question – “Why not try a 2-4 week trial of BCST, which has far superior outcomes for cough, before an empiric 2-3 month trial of a medication?” Of course, the only way that could happen is if BCST became widely available.
Ultimately, early access to BCST would drastically drop rates of long-term chronic cough, which would enable healthcare practitioners to better use their time and save the health system vast sums of unneeded spending.
